





March 2026
In this VETgirl online veterinary continuing education blog, Dr. Amy Kaplan, cVMA, DACVECC, MRCVS explores the evolving landscape of feline infectious peritonitis (FIP), highlighting how antiviral treatments have transformed this once grim diagnosis into a potentially manageable condition. Part 1 of this 2-part series focuses on recognizing FIP’s diverse clinical signs, risk factors, and diagnostic challenges, emphasizing rapid diagnosis to enable early treatment for optimal outcomes.
Check out this VETgirl podcast about all you need to know about FIP heading into 2026 HERE and check out Part-2 HERE!
By Dr. Amy Kaplan-Zattler, cVMA, DACVECC, MRCVS
VETgirl CE Program Manager
FIP Updates From 2025 Part 1: New Data, New Doses, New Hope
For years, feline infectious peritonitis (FIP) had been a diagnosis that made everyone’s stomach drop — the kind of case that felt as grim as the big “C” (cancer) diagnosis. But in the last few years, extra-label use of select antivirals has flipped the script, with reported response rates around 85–90%. With treatment now truly on the table, the priority shifts to rapid, confident diagnosis so cats can start therapy as early as possible for the best outcomes. In Part 1 of this 2-part blog, we focus on recognizing FIP in real life and how to build the strongest supportive diagnostic case. Check back next week for Part 2, where we dive into updated treatment strategies, including dosing, monitoring, and with a refreshed antiviral “cheat sheet” chart.
Which Cats get FIP?
Most young cats will pick up a feline enteric coronavirus (FeCV) at some point – often early in life – especially when living in close proximity of other cats such as in multi-cat households, catteries, or shelters. FeCV replicates within the apical columnar epithelial cells of the small intestine which can cause gastrointestinal signs such as diarrhea, some cats develop upper respiratory signs, and some remain asymptomatic. The virus is shed as early as 2-3 days after infection and cats may continue shedding for up to several weeks; a small handful of cats have been documented to shed lifelong. The diarrhea is usually short-lived, but if you have a kitten presenting with a history of persistent diarrhea for weeks to months, FeCV should definitely be among your differential diagnoses.

Image courtesy of Dr. Dave Gordon
In a small number of cats infected with FeCV (around 10%), the virus can mutate and begin replicating within macrophages and monocytes. At this stage, the newly mutated virus is called the feline infectious peritonitis virus (FIPV) and it essentially “hitchhikes” inside these white blood cells throughout the body, triggering an over-the-top inflammatory response centered around blood vessels (i.e., vasculitis), which is what ultimately drives the clinical symptoms of FIP. We still don’t fully understand how or why this mutation occurs in some cats but not in their siblings or in other cats living in the same environment.
FIP is more often thought as a “young-cat” disease (< 2 years of age), but don’t cross it off your differential list in adult cats; a small percentage are first diagnosed later in life. Intact males are overrepresented compared to females, and breed may also play a role as purebred cats have been overrepresented in some reports. Other risk factors include coinfection with feline immunodeficiency virus (FIV) or feline leukemia virus (FeLV), other concurrent disease, immunosuppression, and stress.
What Does FIP Look Like Clinically in our Feline Patients?
FIP is not a one-size-fits all disease – in fact it’s quite the shape-shifter. Many times FIP presents as an “ADR” cat, producing only nonspecific signs (e.g., lethargy, anorexia, weight loss or failure to gain weight, waxing/waning fever). Check out a list of various clinical signs in the figure at the end of this blog!
Broadly, we talk about two categorizations of FIP: the ‘wet form’ and the ‘dry form.’
- Effusive, or ‘wet’, FIP might look like the pot-bellied cat, or the cat working harder to breathe due to large-volume abdominal fluid compressing/restricting the diaphragm. FIP effusion most commonly accumulates in the abdomen or chest, and occasionally in the pericardial sac or scrotal sac.
- Non-effusive, or ‘dry’, FIP tends to show up as pyogranulomatous lesions in organs like the kidneys, liver, lymph nodes (including mesenteric lymph nodes), and in the eyes and brain.


Bullous keratopathy in an FIP positive cat. While this cat’s bullous keratopathy may have been idiopathic in origin or linked to other factors, it’s possible this was caused from progression of severe anterior uveitis and corneal edema secondary to FIPV. (Image courtesy of Dr. Amy Kaplan, cVMA, DACVECC, MRCVS)
Neurologic signs reflect the neuroanatomic distribution of disease, which may be focal, multifocal, or diffuse and can be seen as clinical signs of:

And because FIP doesn’t follow the book, cats can present with mixed-form FIP showing clinical features attributed to both ‘wet’ and ‘dry’ forms. Regardless of the form, cats may also develop jaundice, lymphadenopathy, or pale mucous membranes. Less common manifestations include pruritic nodules or papules and other dermatologic changes, as well as glomerulonephritis due to immune-complex deposition. For these reasons, separating FIP into ‘wet’ and ‘dry’ forms is not particularly useful, because they do not represent distinct disease entities. However, the patient’s clinical signs can help guide our selection of diagnostic tools, and can help identify which treatment protocols to follow.
Diagnostic Dilemma – Support vs. Confirmation
Diagnosing FIP can be frustrating, especially in dry (non-effusive) cases where you don’t have biopsy results or the benefit of an accessible and diagnostically useful effusion sample. The clinical signs of FIP are often nonspecific and many readily available tests in practice provide diagnostic support rather than confirmation of FIP. The gold standard for confirmation remains immunohistochemistry (IHC) demonstrating FIP viral antigen within macrophages, typically performed on tissue samples obtained via laparoscopy, laparotomy, or post-mortem examination. If ocular involvement is present, aqueous humor can also be submitted for IHC. In real life, however, IHC isn’t always feasible in a timely manner, so clinicians commonly rely on a layered approach of stacking supportive findings until the overall clinical picture is compelling enough to justify treatment.
When FIP is on the differential list, it’s best to start with baseline diagnostics: a complete blood count (CBC), serum biochemistry, urinalysis (to assess for possible renal involvement), and FeLV/FIV testing.
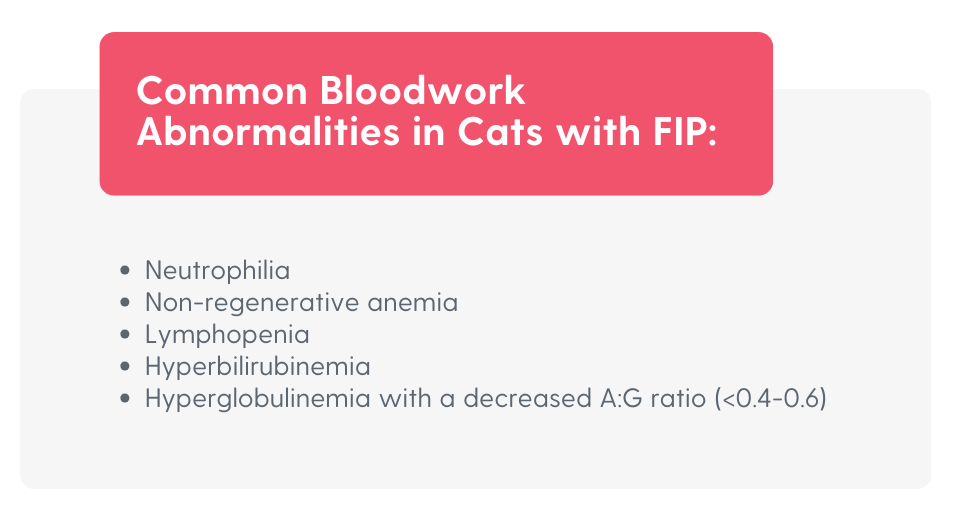
The albumin-to-globulin (A:G) ratio is calculated from measured albumin and globulin concentrations in serum/plasma or effusion. In cats with FIP, a low A:G ratio reflects the classic combination of polyclonal hyperglobulinemia (chronic immune stimulation/inflammation) and hypoalbuminemia (negative acute-phase response, decreased production during inflammation, and/or redistribution). Clinically, this is supportive but not diagnostic, because other inflammatory, infectious, and neoplastic diseases can produce a similar pattern.

Next, if an effusion is identified, the diagnostic workup should “pivot” toward effusion characterization and targeted effusion tests, because FIP effusions often carry higher-yield clues. While variability of the clinical features exists (and concurrent disease can muddy the waters), FIP-associated effusions commonly share these features:
- Color: yellow/amber/straw; transparent to cloudy
- Texture: viscous (“sticky”)
- Protein: typically >3.5 g/dL (>35 g/L)
- Cellularity: often low, but variable (approximately 2–6 × 10³/µL, sometimes higher); commonly non-degenerate neutrophils and macrophages with fewer lymphocytes and a granular proteinaceous background
- Effusion A:G ratio: often <0.4

Viscus, “stringy” fluid sampled from a kitten’s abdomen with suspected FIP based on clinicopathologic support. (Image courtesy of Dr. Amy Kaplan, cVMA, DACVECC, MRCVS)
RT-qPCR on effusion is often treated as a “heavy hitter” because published performance can be excellent, and it’s fast enough to fit into clinical workflows, but it’s limited by cost, equipment, and technical expertise, which can make routine access variable.
Rivalta’s test is a simple, low-cost bedside assay performed on effusion fluid that can be a helpful piece of the diagnostic puzzle for FIP. It evaluates whether the effusion contains a high concentration of protein and inflammatory macromolecules (classically including fibrin/fibrinogen), which will precipitate when exposed to dilute acetic acid. To perform the test, prepare a dilute acetic acid solution by adding 20–30 µL of 98% acetic acid to 7–8 mL of distilled water in a plain, sterile test tube (no additives), then gently place a single drop of effusion onto the surface of the solution in the tube.

(Video courtesy of Dr. Dave Gordon)
The catch? This visible reaction isn’t exclusive to FIP; a positive Rivalta’s test can also be seen with bacterial peritonitis, pleuritis, or lymphoma. A negative Rivalta’s test, however, may help to rule out FIP. Bottom line: don’t rely on a positive Rivalta’s test alone. Instead, interpret it alongside cytologic findings and the patient’s overall clinical picture.
More recently, delta total nucleated cell count (ΔTNC) has been investigated as an objective, analyzer-based method to support a diagnosis of FIP in cats with effusion. Lopes et al., describe the underlying principle that many FIP effusions are markedly protein-rich, and when they are processed through certain automated hematology analyzers, the BASO reagent channel can promote fibrin clot formation. These micro clots then physically entrap nucleated cells from the sample, resulting in an artificially low nucleated cell count within the BASO channel, as compared to the other channels. The magnitude of this discrepancy in nucleated cell counts between channels is reported as the ΔTNC, and larger values (i.e., larger discrepancies in cell counts) supports a diagnosis of FIP.
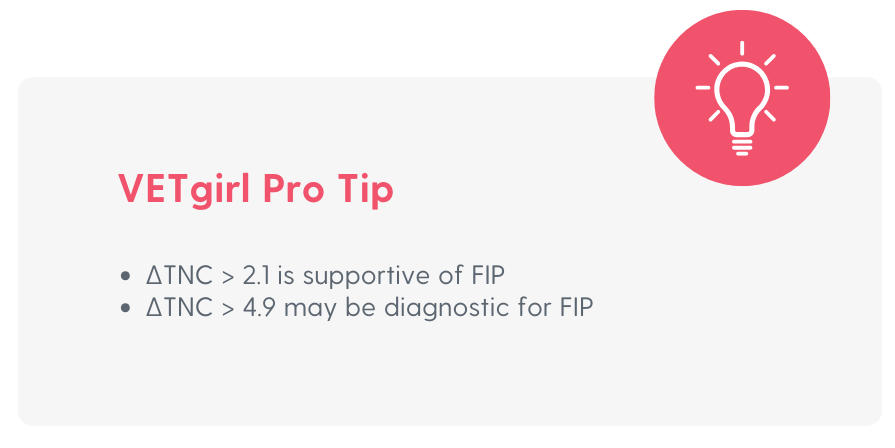
Conceptually, the ΔTNC is similar to Rivalta’s test (both are indirectly demonstrating that an effusion is unusually high in protein). However, ΔTNC is typically considered a more objective diagnostic because it’s machine-quantified and less prone to inter-observer variability. It has also shown improved differentiation of FIP effusions from some septic and neoplastic effusions compared with Rivalta’s and A:G alone.
If you want to push diagnostic confidence even further, the FIP Effusion Index combines two complementary signals, capturing both the inflammatory ‘protein signature’ and the effusion’s ‘cellular behavior’ in one value:
- Protein pattern (A:G) and
- Cellular behavior (ΔTNC)
The FIP Effusion Index is calculated by dividing the ΔTNC by the A:G, meaning it increases when ΔTNC is higher and/or the A:G ratio is lower, with a higher result being supportive of FIP.
Conclusion
FIP workups are less about chasing certainty and more about making high-quality decisions with the data you can realistically get – think pattern recognition + smart sampling. Baseline labs can raise (or lower) suspicion, but when effusion is present it becomes your diagnostic MVP. Your endgame is clinical confidence: enough evidence to move forward quickly, explain your reasoning clearly to clients, and start therapy without unnecessary delays. Come back next week to check out Part 2: the treatment playbook — what to use, how to dose, how to monitor, and how to handle FIP relapses.
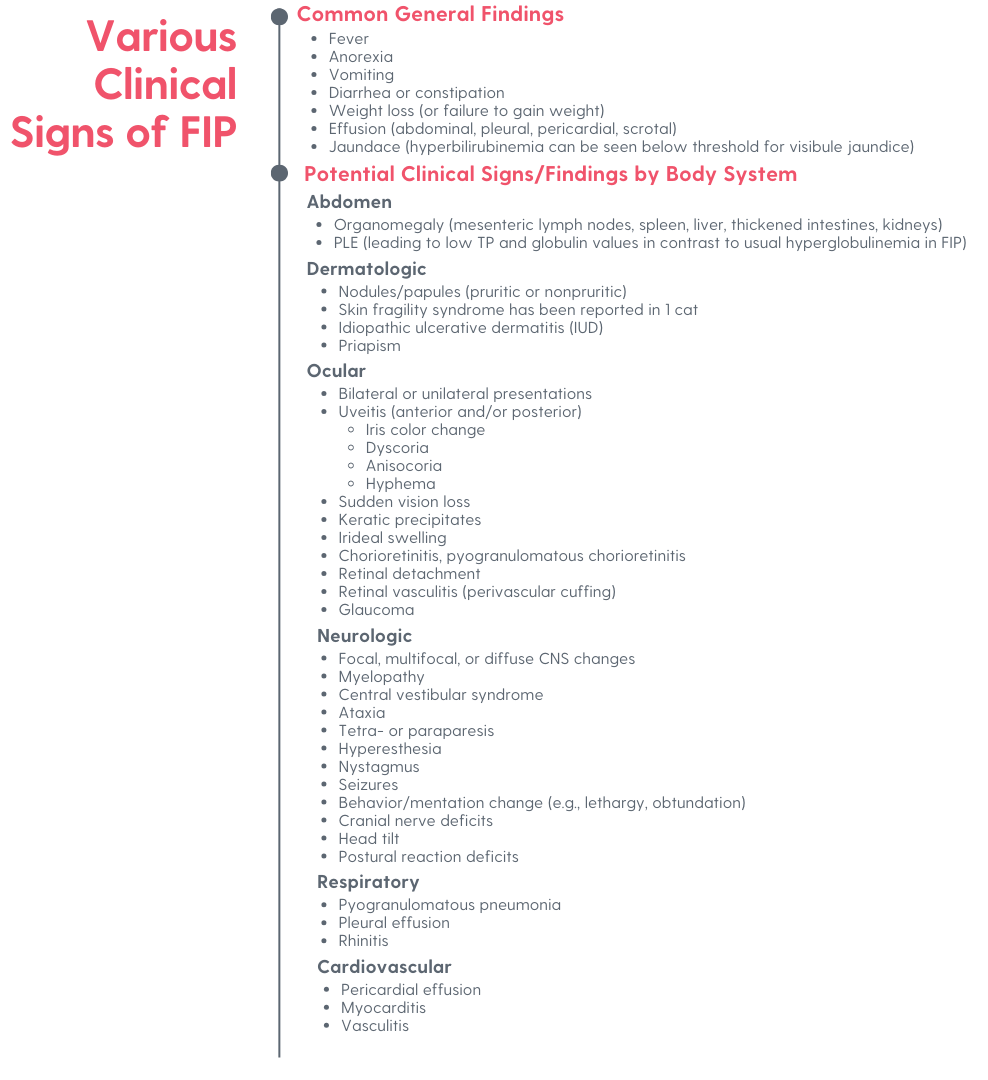
Figure 1.
Abbreviations:
A:G: albumin-to-globulin ratio; also abbreviated as A/G, AG, AGR
ADR: “ain’t doin right”
CBC: cell blood count
FCoV: feline coronavirus
FeCV: feline enteric coronavirus
FeLV: feline leukemia virus
FIP: feline infectious peritonitis
FIPV: feline infectious peritonitis virus
FIV: feline immunodeficiency virus
IHC: immunohistochemistry
MVP: most valuable player
RT-qPCR: quantitative reverse transcription PCR
ΔTNC: delta total nucleated cell count
References:
- Taylor S, Tasker S, Barker E, et al. An update on the treatment of feline infectious peritonitis (July 2025). International Cat Care; Accessed January 26, 2026.
- Tasker S, Addie DD, Egberink H, et al. Feline Infectious Peritonitis: European Advisory Board on Cat Diseases Guidelines. Viruses. 2023;15(9):1847. doi: 10.3390/v15091847.
- Andrews ALMM, Izaguirre E, Green J, et al. Treatment With Remdesivir Alone or in Combination With GS-441524 in Cats With Ocular Involvement of Feline Infectious Peritonitis: An Observational Case Series. J Vet Intern Med. 2025;39(6):e70253.
- Roman N. Feline infectious peritonitis. Merck Veterinary Manual. Updated November 2025. Accessed January 26, 2026.
- Lopes R, Sampaio F, Carvalho HL, et al. Feline Infectious Peritonitis Effusion Index: A Novel Diagnostic Method and Validation of Flow Cytometry-Based Delta Total Nucleated Cells Analysis on the Sysmex XN-1000V®. Vet Sci. 2024;11(11):563.
- Thayer V, Gogolski S, Felten S, et al. 2022 AAFP/Every Cat Feline Infectious Peritonitis Diagnosis Guidelines. J Feline Med Surg. 2022;24(9):905-933. doi: 10.1177/1098612X221118761.




Only VETgirl members can leave comments. Sign In or Join VETgirl now!