




December 2025
In this VETgirl online veterinary continuing education blog, Dr. Amy Kaplan, cVMA, DACVECC, MRCVS details what to do when faced with a bleeding veterinary patient. It’s easy to feel overwhelmed. Is it the platelets or is it clotting factors? Or is the whole system just falling apart? This is where coagulation testing can help us find focus. In Part 1 of this VETgirl veterinary CE blog, we talked about blood products and how to pick the right bag for the right patient, so make sure to go back and read that part first HERE. In Part 2, we’re flipping to coag diagnostics — figuring out which part of hemostasis is failing so you can target your treatments and stop the bleed in that critically ill or emergent dog or cat.
Veterinary Transfusion Medicine 101 Part 2: How to Interpret Coagulation Tests in Dogs and Cats
Dr. Amy Kaplan, cVMA, DACVECC, MRCVS, CE Program Manager, VETgirl
In Part 1, we tackled blood products: what’s in the bag, how long they last, and when to use them. But knowing your products is only half the battle. (If you haven’t already read that part first, make sure to check it out HERE). Before we can choose the right blood product, we have to know why our patient is bleeding in the first place. That’s where coagulation testing comes in. From the simple in-house screening tests to advanced viscoelastic assays, let’s walk through the most commonly used coagulation tests, what they actually measure, and how to apply them at the bedside. (P.S. If you want quick-access to easy-to-use visual charts, check out our Clinical Transfusion Essentials Toolkit and grab your free download today!)
Recognizing Patient Hemorrhage
First, we need to have a hunch that our patient is bleeding, which truly isn’t always obvious! Sure, sometimes you’re staring at a pool of bloody vomit, but other times the bleed can be more subtle — a new bruise, a hematoma, petechia or ecchymosis, pallor, or in severe cases, sudden collapse. Careful physical examination and close monitoring are your first screening tools.

Primary vs. Secondary Hemostasis: Where Does the Coagulation Disorder Begin?
The first task is to determine which of the 3 main hemostatic systems needs help:

This chart’s a handy guide to help sharpen your clinical eye and prioritize testing, but remember — clinical signs can overlap hemostatic systems, so use this chart only as a general guideline and consider this information against your clinical patient assessment. A pragmatic, stepwise approach to coagulopathies is often the best way forward.
Understanding Platelet Counts and Function
Petechiae? Think “P” for platelets. But even without them, any concern for bleeding should start with a platelet count — it’s a quick, essential first step.
The catch? Automated analyzers can be fooled by platelet clumping, giving you an artificially low count. So, if results look suspicious, trust your own eyeballs — make a smear, scan the feathered edge to check for platelet clumps that will skew automated and manual counts, and then find the blood film’s monolayer to perform a manual platelet estimate over 10 high-power fields. QUICK TIP: roughly, one platelet per hpf equals about 15,000/µL.
True spontaneous bleeding usually doesn’t occur until platelet counts drop below roughly 20–25,000/µL. That said, there are always exceptions. Cytokines and inflammatory mediators released during surgery, vasculitis, infection, autoimmune disease, trauma, or the concurrent use of certain medications (e.g., NSAIDs, colloids), can impair normal platelet function — so a patient may still spontaneously bleed even with counts in the 35,000–50,000/µL range.
When platelet numbers look fine but you’re still seeing evidence of bleeding, it’s time to ask how well those platelets are actually working. The Buccal Mucosal Bleeding Time (BMBT) is a simple — if slightly crude — way to assess how effectively an initial platelet plug forms. (NOTE: BMBT can be artificially prolonged by thrombocytopenia – another reason to check a platelet count first!) In this test, a small, standardized cut is made on the buccal surface of the lip, and you measure how long it takes for bleeding to stop while gently wicking away excess blood (to avoid pooling or “streaming” that can skew results). Normal BMBT times are <4 minutes in dogs and <2.5 minutes in cats. If platelet counts are normal but the BMBT is prolonged, think von Willebrand disease or platelet dysfunction — but don’t forget that NSAIDs and uremia from renal failure can also impair platelet function and potentially stretch out those bleeding times. Looking for a quick refresher on how to perform a BMBT? Check out this VETgirl video: How to perform a buccal mucosal bleeding time (BMBT) in a dog.
Photo courtesy of VETgirl
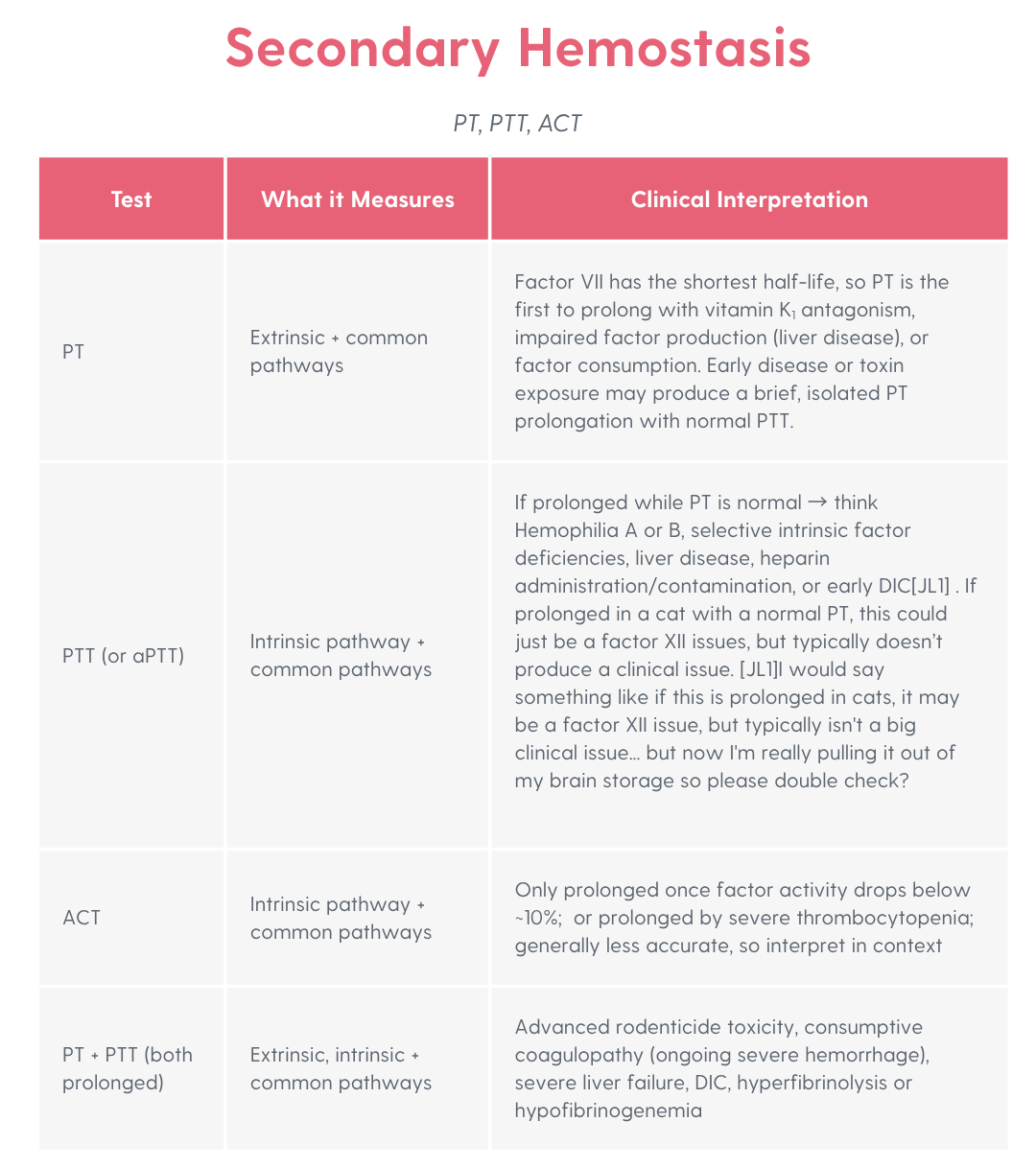
Secondary Hemostasis: PT, PTT, and ACT
Secondary hemostasis is all about the clotting cascade — those numbered factors that stabilize fibrin clots and probably are stirring up flashbacks from vet school PowerPoints. Yup, you actually still need to remember some key points of that coag cascade! The main screening tests here are prothrombin time (PT), partial thromboplastin time (PTT), and activated clotting time (ACT). These tests typically test for hypocoagulability (e.g., prolonged clotting).
Most hospitals will have either a PTT or an ACT, since both assess the intrinsic and common pathways. The difference? PTT is more sensitive, while ACT is the quick, cheap, cage-side option (Any test that you have to put in your armpit to measure the number of seconds till initial clot formation isn’t all that accurate, but at least it’s something!).
Keep in mind: PT and PTT become prolonged once a factor or multiple factors’ activity drops below approximately 25-30% of normal, but ACT won’t show a change until activity falls below roughly 10%. And here’s another catch — while PT and PTT aren’t affected by platelet numbers, ACT can be falsely prolonged in cases of severe thrombocytopenia. Just one more reason to check those platelets first; in other words, if your patient is thrombocytopenic, don’t bother doing an ACT. That said, please note that your PT and PTT will never be affected by thrombocytopenia unless there is truly a clotting factor issue or underlying disease process (e.g., DIC).
More Tests to Round Out the Picture
Sometimes your frontline tests — BMBT, PT, PTT, and ACT — don’t tell the whole story. When the basics leave you scratching your head, additional assays can help you zero in on whether the issue lies with fibrinogen (clot formation), fibrinolysis (clot breakdown), or overall clot stability. These tests usually need to be sent out to a reference lab, so results won’t be instant — but the info can be game-changing when managing tricky coagulopathies.
Thrombin Time (TT)
Thrombin time looks at the final step of the clotting process — when thrombin converts fibrinogen (soluble) into fibrin (insoluble). Thrombin is added to plasma, and the time to clot formation is recorded. A prolonged TT can mean low, absent, or dysfunctional fibrinogen, or interference (e.g., heparin use, contamination).
Fibrinogen Activity
This test evaluates whether there’s enough substrate to form a stable clot. Specifically, it measures the patient’s level of functional fibrinogen. In the common pathway, thrombin cleaves fibrinogen into fibrin monomers, which then polymerize into long fibrin strands. Factor XIII (fibrin stabilizing factor), also activated by thrombin, cross-links those fibrin strands to stabilize the clot.
In the fibrinogen activity test, an excessive amount of thrombin is added to the patient’s plasma. By flooding the sample with thrombin, we make sure any delay or weakness in clot formation reflects a problem with the fibrinogen itself — not a thrombin deficiency. The recorded clotting time is inversely correlated with the patient’s fibrinogen concentration.
Low fibrinogen levels can indicate liver failure, DIC, congenital deficiencies, or severe malnutrition. Elevated fibrinogen is often linked to inflammation, infection, pregnancy, or cardiac disease, and may signal an increased thrombotic risk.
Pairing TT with fibrinogen activity (fibrinogen levels) also reveals clinically useful trends:
- Prolonged TT + fibrinogen = hypofibrinogenemia
- Prolonged TT + normal fibrinogen = dysfibrinogenemia
Fibrin degradation products (FDPs) and D-dimers
Think of FDPs and D-dimers as the breadcrumbs left behind when clots are broken down. FDPs reflect the general breakdown of fibrinogen or fibrin, whether or not a stable clot ever fully formed. D-dimers, on the other hand, are more specific — they’re only produced when cross-linked fibrin (the stabilized form of a clot) gets degraded.
That distinction makes D-dimers more clinically useful. Elevated D-dimer levels tell you that fibrinolysis of fully formed cross-linked clots is occurring. Conditions commonly associated with increased D-dimers include DIC, hyperfibrinolysis, and thromboembolic disease (e.g., pulmonary embolism).
But here’s the catch — interpretation isn’t always straightforward. A high D-dimer doesn’t necessarily mean there’s a problem with fibrinolysis; these tests are nonspecific. D-dimers can also rise in situations where excessive clot formation is happening, and fibrinolysis is simply the normal physiologic response — like with trauma, inflammation, or post-surgical recovery. So be sure to always interpret D-dimer results in the broader clinical context!
Viscoelastic Testing
If you’re still scratching your head about how to put these results together, viscoelastic testing offers a one-stop-shop approach with its global, real-time view of clot formation, strength, and breakdown (lysis). Thromboelastography (TEG) and rotational thromboelastometry (ROTEM) are 2 distinct viscoelastic testing methods that can identify both bleeding tendencies and hypercoagulable states (e.g., clotting too quickly) all in one test. While these tests are still most commonly found in referral centers and veterinary diagnostic laboratories, portable systems are becoming more available. As access improves, viscoelastic testing has the potential to reshape how we diagnose and manage coagulopathies in everyday practice.

Coagulation testing can feel messy, but it doesn’t need to make your head spin. Approach these tests in stepwise fashion, understand what the tests can (and can’t) tell you, and when in doubt, phone a friend – a clinical pathologist, diagnostic lab, or your local go-to criticalist or internist, too!
VETgirl Takeaways
- Look before you lab: if we aren’t looking at our patients, we won’t detect the early clinical signs of hemorrhage.
- ‘P’ for platelets: as a generality (so not in all cases!) petechiae means platelets. Confirm low counts on a smear — clumping can fool analyzers. True spontaneous bleeding is uncommon until platelets are <20–25K/µL, but platelet dysfunction can tip patients into a bleeding crisis at higher counts.
- Coag Screen Team: PT, PTT, and ACT are your frontline screening tests for secondary hemostasis. PTT and PT are not impacted by severe thrombocytopenia, whereas ACT is artifactually prolonged.
- Additional tests: add on a TT, fibrinogen, and D-dimers to add more context when basic coagulation tests don’t provide enough. Always interpret results alongside the patient and other data (especially with those non-specific D-dimers).
- Look at the Big Picture: viscoelastic testing (TEG/ROTEM) gives a global picture of clot formation, strength, and breakdown and access is becoming more available in large ER and referral hospitals.
Bottom line: Pair clinical signs with the right test, know each test’s limitations, and always interpret results in clinical context using a stepwise, pragmatic approach.
Want this info at your fingertips for when you need it fast? Download our Coagulation Test Interpretation Guide from the Clinical Transfusion Essentials Toolkit today!
Abbreviations:
ACT: Activated Clotting Time
BMBT: Buccal Mucosal Bleeding Time
DIC: Disseminated Intravascular Coagulation
FDPs: Fibrin Degradation Products
PT: Prothrombin Time
PTE: Pulmonary Thromboembolism
PTT: Partial Thromboplastin Time (often used interchangeably with aPTT, Activated Partial Thromboplastin Time)
ROTEM: Rotational Thromboelastometry
TEG: Thromboelastography
TT: Thrombin Time
vWF: von Willebrand Factor
References:
- Silverstein DC, Hopper K, editors. Small Animal Critical Care Medicine. 1st ed. St. Louis, MO. Saunders Elsevier; 2009:510.
- eclinpath.com, Cornell University College of Veterinary Medicine, https://eclinpath.com/hemostasis/tests/screening-coagulation-assays, accessed August 5, 2025.
- Herring J, McMichael M. Diagnostic approach to small animal bleeding disorders. Top Companion Anim Med. 2012;27(2):73-80.



Only VETgirl members can leave comments. Sign In or Join VETgirl now!